
Updated July 2026
The RCGP continues to engage with NHS England and other stakeholders on the implementation and development of Advice and Guidance (A&G) and elective Single Point of Access (SPoA) models in England.
Advice and Guidance has the potential to improve patient care by enabling timely access to specialist expertise and supporting collaboration between primary and secondary care. Its success depends not simply on increasing its use, but on the quality, timeliness and consistency of specialist advice, and on ensuring that patients can access specialist assessment promptly whenever it is clinically indicated.
Following concerns raised by the RCGP and others, NHS England have provided further guidance for GPs and patients. Important clarifications include that:
- The introduction of elective Single Points of Access (SPoA) is intended to support timely specialist assessment and improve referral pathways, not to reduce or refuse clinically appropriate referrals.
- Referral thresholds remain unchanged, there is no 25% national target to divert referrals away from secondary care (as previously reported), and GPs should continue to refer where specialist care is in the patient's best interests.
- Secondary care consultants are expected to provide timely, named consultant-led responses: action routine referrals within 5 working days, urgent referrals within 2 working days, and respond to specialist advice requests within 5 working days of receipt, with a clear next step for the patient's care.
- Responsibilities for arranging, reviewing and acting on specialist diagnostics sits with secondary care as part of the specialised pathway.
- Systems should be co-designed in collaboration between trusts, Integrated Care Boards (ICBs) and general practice. General practice remains responsible only for diagnostic tests that are routinely undertaken as part of initial assessment or prior to referral.
The College has welcomed these clarifications, in particular that there will be no target to divert 25% of referrals from hospital care and that all referrals will be reviewed by a specialist consultant. Such a target would have undermined clinical decision-making, increased workload in general practice and created barriers to timely patient care.
However, many GPs continue to report concerns about local implementation, including variable pathways, additional workload, inconsistent interpretation of responsibilities between primary and secondary care, and whether patients are always able to access timely specialist assessment when clinically indicated.
It is critical that reforms are properly resourced, avoid shifting additional workload onto general practice, protect patient choice and clinical autonomy, and are subject to ongoing evaluation to ensure they improve patient outcomes without widening inequalities or creating unintended consequences.
The College will continue to monitor the implementation, gather feedback from members and work with NHS England and other stakeholders to ensure that A&G delivers timely access to specialist expertise, protects patient care and clinical autonomy, maintains appropriate professional responsibilities, and does not result in inappropriate or unfunded transfer of workload into general practice.
Our latest press release
- RCGP welcomes NHS England’s move away from rigid A&G target (published 23rd April 2026)
Updated March 2026
Key developments indicate a national direction of travel that seeks to increase the use of Advice and Guidance (A&G) in England.
The Medium Term Planning Framework (published October 2025) asks general practice to continue prioritising the use of A&G before, or instead of, making a planned care referral, where clinically appropriate and excluding referrals for urgent suspected cancer. The guidance sets out ambitions for all referrals to go via A&G, for the 10 specialties at provider level which have the most potential for this model to be effective, supported and delivered through ICB-led strategic commissioning. Alongside these aims, and expectations for all requests to flow through e-Referral Service (e-RS) by July 2026, the framework encourages systems to ensure all referrals receive appropriate clinical triage.
Similarly, changes to the GP Contract in England for 2026/27 include plans to amend the contract to embed the current Advice and Guidance (A&G) Enhanced Service funding (£82million) within core practice funding. Practices will be required to use A&G prior to or in place of a planned care referral where clinically appropriate and to follow locally agreed referral pathways, including single point of access models (SPoA) once introduced.
It remains the RCGP’s long-standing position that the use of A&G should not be mandated in any area.
The College recently published a press response the 2026/27 GP contract announcement, highlighting the need to be cautious of how A&G is integrated into the GP contract and the implementation of a SPoA model for all specialist referrals. While we support plans to shift care from hospital into the community where appropriate, sufficient investment has to follow if GPs are going to be able to deliver safe, timely care close to home. Advice and Guidance can be a useful way for GPs to seek timely specialist input for patients, and when resourced and implemented appropriately, it has the potential to support more joined-up care across the NHS. However, local pathways involving its use must be carefully co-designed by primary and secondary care, alongside patients, to ensure they work effectively for patients and clinicians.
Our members report that there are already significant differences in A&G processes across the country. There is legitimate concern that areas where secondary care waiting lists are highest may experience greater use of A&G under a SPoA approach, as a means of managing pressure on secondary care services, with potential negative impacts on patient experiences, outcomes, quality of care, and stability of local GP practices. There are ongoing concerns that A&G facilitates a significant shift of workload from secondary care which is not fully resourced, even with the additional funding that has been available. The average number of monthly A&G requests are rising significantly, having nearly doubled over the period of April 2022 to January 2026. It is crucial that the funding matches the workload and that this funding increases appropriately in line with increases in use of A&G.
Further, it is not fully clear how a SPoA would work in practice across the country, and one approach may not be suitable in all areas. Our members have raised concerns over how its use varies across the country, how delays and potentially blocked referrals can jeopardise patient safety, and how it can push workload from secondary to primary care without clear resourcing, consistent clinical governance, or sufficient consideration of the downstream consequences for GP capacity and the quality-of-care patients receive. An SPoA approach must not delay or limit appropriate referrals or impose ways of working that are not safe or suitable for patients or for general practice.
A shift to this approach is likely to require further discussion and piloting before it is implemented, and therefore may not be feasible for full national implementation in 26/27 without further evaluation. We have heard reports of risks of delays with tests being required before any referral, lost messages and staff without appropriate senior clinical oversight handling requests. If a SPoA approach is to be implemented, it is even more crucial that it is mandated that requests are assessed by secondary care Consultants only. It is important that there are co-designed clinical pathways of care, that consider the complex whole-person context, and that workload does not transfer to general practice without relevant resources.
The College will continue to raise our concerns with NHSE and DHSC, working closely with system partners, including the BMA on contractual matters, to support GPs and their teams.
Our latest press release
- RCGP responds to GP contract announcement (published 24 February 2026)
- ‘Funding must follow the patient’, College welcomes support for Advice and Guidance services (published 17 April 2025)
- Funding A&G services ‘a good step’ – RCGP responds to elective care plan (published 06 January 2025)
Updated April 2025
From 1 April 2025, NHS England have introduced the formal General Practice Requests for Advice and Guidance Enhanced Service (A&G ES), as part of wider changes to the national 2025/26 GP Contract in England. Backed by up to £80 million in funding, the ES encourages GPs to seek specialist advice pre-referral, with a £20 Item of Service (IoS) payment for each request to recognise the additional workload created for general practice. The RCGP welcomes this step, while emphasising the need for appropriate resourcing and investment in general practice to deliver A&G consistently across the country to support timely, safe, and appropriate care of our patients close to home.
The RCGP and BMA have worked with NHSE/I on guidance relating to the Advice and Guidance initiative, with direct access to investigations, to produce specialist advice clinical responsibility FAQs and specialist advice Medico-legal FAQs.
Further specifics of the service, as of April 2025
Advice and Guidance (A&G) is a non-face-to-face, GP-led enhanced service within England that supports general practice teams to seek specialist advice from secondary care before, or instead of making a referral. It enables clinical dialogue between GPs and consultants to support non-urgent patient care, particularly in cases of diagnostic uncertainty or where referral thresholds may not be met. The types of advice that may be requested include, but are not limited to, treatment plans, interpretation of results and/or advice on appropriateness of referrals/tests.
Joint guidance on the NHS e-Referral Service (e-RS) developed by GPC England, NHS England, and NHS Digital notes that when properly implemented, the e-RS A&G feature ‘allows a multi-way conversation to take place between GPs and Consultants that can help strengthen professional relationships, share knowledge and promote important clinician-to-clinician dialogue around patient care’.
The government aims to increase pre-referral advice requests from GPs to up to four million in 2025/26 (up from 2.4 million in 2023/24) as part of wider efforts to cut waiting lists and improve patient care.
All GP practices – whether operating under a GMS contract, PMS agreement or APMS contract – are eligible to opt in to the enhanced service, provided they meet the specified requirements. In 2022, the RCGP recommended that A&G should be optional and not mandated, and we are glad to see that participation is voluntary on an opt-in basis.
A&G can be delivered in real-time/synchronously (e.g. telephone) or asynchronously (e.g. NHS e-Referral Service (e-RS) or secure email).
A&G requests can be non-specific, they are not a prerequisite to formal referral, and do not start a referral-to-treatment (RTT) clock.
Practices can claim a £20 Item of Service (IoS) payment for each GP-led pre-referral A&G request, including all related follow-up activity within a single episode.
At a local level, Integrated Care Boards (ICBs) may introduce caps on claimable A&G activity per practice, to stay within the national £80 million budget for 2025/26. Practices can submit additional requests beyond the cap, but they will not be reimbursed.
Full details can be found within NHS England’s Enhanced Service Specification for General Practice Requests for Advice and Guidance 2025/26.
Our latest press responses
‘Funding must follow the patient’, College welcomes support for Advice and Guidance services (published 17 April 2025)
Funding A&G services ‘a good step’ – RCGP responds to elective care plan (published 06 January 2025)
Updated May 2022
NHS Digital states that NHS e referral service (e-RS) advice and guidance (A&G) “is a two-way dialogue channel in the e-RS which allows GPs/referrers to seek specialist input into a patient’s care” providing “a secure rapid digital communication channel between two clinicians, the ‘requesting’ clinician and the provider of a service (the ‘responding’ clinician), enabling a patient’s care to be managed in the most appropriate setting”.
NHS Digital states that there “may be a number of reasons why a clinician may wish to use the service including:
- asking another clinician or specialist for their advice on a treatment plan and/or the ongoing management of a patient
- clarification (or advice) regarding a patient’s test results
- seeking advice on the appropriateness of a referral for their patient (e.g. whether to refer, or what the most appropriate alternative care pathway might be)
- identifying the most clinically appropriate service to refer a patient in to”
Since February 2021 the E-RS advice and guidance was amended, aiming to “reduce the burden on GPs/referrers”, by allowing “advice and guidance to be used as a referral channel”, thus preventing information passing back and forward between the requesting and responding clinician aiming to “streamline patient care”.
As a result of the pandemic and the backlog of care, there are now over 6.1 million people waiting for treatment after referral in England. Published data from February 2022 shows record numbers of people waiting, with over 2 million waiting longer than 18 weeks and 300,000 waiting longer than 1 year for treatment and the average waiting time being 13.1 weeks. At the same time, the number of primary care referrals to secondary care that were rejected, increased by 87% (from 238,859 in February 2020 before the pandemic began, to 401115 in November 2021).
When GP referrals are delayed or rejected, patient care does not end. These people and their carers are held in the community, cared for by primary care. This is increasing the workload pressure within the community and creating a backlog of care in general practice.
The RCGP understand that advice and guidance is being used by some providers to manage their waiting lists, (such as converting requests to referral to advice and guidance or using advice and guidance to decline referrals) which in some areas, is adding increased workload burden to primary care.
A recent survey (April 2022) of RCGP clinical advisers showed that almost all GPs (91.7%) used advice and guidance, with the vast majority (83%) finding it useful. Examples were given of rapid responses to questions that were helpful in streamlining patient care. The response times and quality of responses varied depending upon the individual clinician, specialty and geography; with some respondents stating that there were unacceptable delays in gaining answers to questions necessitating increased holding of risk and patient care delays within primary care.
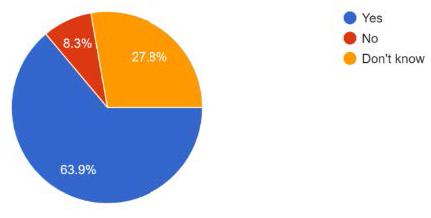
64% of respondents believe that the advice and guidance was being used as a referral management tool, aiming to reduce referrals into secondary care. Whilst it is accepted that A&G is a useful tool to reduce referrals to secondary care of patients who could be equally well managed in primary or community care settings, there is significant concern in our survey that the responses from secondary care were sometimes asking for unrealistic investigations to be performed by primary care, many of which are not available in the community, and would ordinarily have been requested within secondary care, at or prior to the outpatient appointment post referral. In addition, there were increasing numbers of referrals being rejected and converted to A&G offering advice on management within the community, rather than seeing the patient in secondary care.
Is A&G being used to reduce referrals in your area?
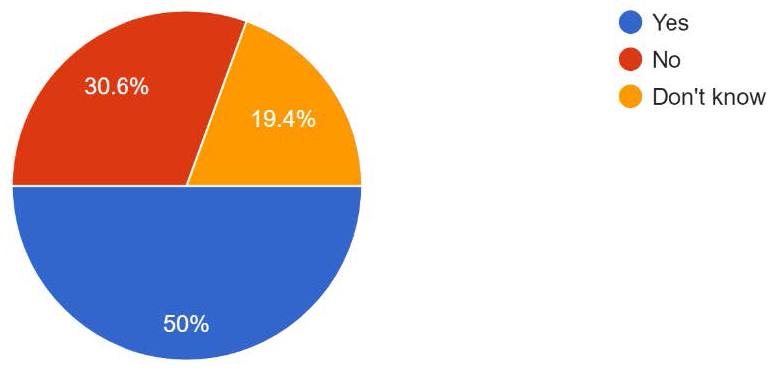
There is variability across the system in terms of the impact on GP workload. 50% of respondents believed A&G increased workload within primary care, because it was used as a way to move the initiation of investigations and treatment into primary care that would ordinarily be commenced in secondary care. This led to some respondents describing having to treat conditions that they felt outside of their clinical competence based on A&G responses.
Whilst NHS Digital states the aim of the service since the changes in February 2021, are to “reduce the burden on GPs/referrers”, by allowing “advice and guidance to be used as a referral channel”, our survey has found in some areas the opposite is happening. A&G is being used by some providers to hold a conversation between clinicians, rather than accepting the referral requested by primary care. It was noted that this then increases the workload within general practice as for every A&G response, the primary care team needs to book a further patient appointment, and if further questions are raised, create another A&G request. The concern is that this may lead to delays in diagnosis, treatment, and increased numbers of primary care consultations when referrals are rejected and then converted to A&G instead.
30% of respondents, however, did not believe it increased workload instead finding the service useful in streamlining patient care, improving access to expert advice and improving knowledge of primary care teams.
Does' Advice and Guidance' increase your workload?
If a patient is referred to secondary care, the clinical risk is then held by secondary care. If a referral is declined, in favour of A&G, then clarification of where the clinical risk lies is required. The RCGP believes the clinical risk should be shared between the clinicians in primary and secondary care and not lie solely in primary care.
In some areas of the country, there are IT issues meaning GPs must log into the secondary care system to continually check for A&G responses, increasing the administrative burden on practices. This is not universal.
Some GPs commented that there was no identifiable clinician on their A&G responses and so if further questions arose, there was no consistent clinical contact available. This also makes it difficult to trust the advice being given, without understanding the level of the advisers. It is essential that any clinical decision made in primary or secondary care follows GMC guidance on good record keeping, identifying the person who gave the advice or made the clinical decision.
- Further support for collaboration between primary and secondary care is essential to enable the backlog of care exacerbated as a result of the pandemic to be managed and streamline patient care.
- If work is to be transferred from secondary to primary care, via A&G, then resource (time, money and people) must follow the patient and not stay in secondary care.
- A&G should be optional and not mandated.
- Other tools to promote closer working between primary and secondary care aiming to streamline patient care are available and should be considered by providers as alternatives, allowing choice. These include direct telephone calls, emails, teledermatology and commercial apps that are able to connect primary and secondary care.
- Clinical care governance and risk must be shared between primary and secondary care during A&G conversations, and this must be understood by all clinicians and their patients when A&G is used.
- When using A&G, all clinicians must uphold the standards of good medical record keeping as per GMC advice, documenting decisions and actions, identifying who has made the decisions and is agreeing with the actions, in the patient clinical record. This should apply to both primary and secondary care and not rely solely on primary care updating the clinical records.
Thank you for your feedback. Your response will help improve this page.