
Banner image: Rover safety bicycle of 1885, © The Board of Trustees of the Science Museum.
Away from the support of the surgery, the GP's bag provided a lifeline to the daily challenges they would face. Before the doctor could even visit a patient, travel, communication and more would all provide their own challenges. A GP's catchment area could take in huge areas, including the city and countryside. It is little wonder urban doctors were often early adopters of the bicycle.
Getting ready for a home visit provided its own challenges. Not knowing what each situation might be, a doctor had to come prepared for as many eventualities as possible. A well-organised doctor’s bag was essential, carrying as many solutions and tools as practically possible. These challenges were often amplified in rural areas, where waiting for additional equipment meant a world of difference to a patient’s outcomes.
Having arrived at the home or bedside, the challenges continued. Outside the surgery, a situation at the home of a patient could be unpredictable with issues of light, space or more. A survey in 1967 found a quarter of homes still lacked internal plumbing. A bag of tricks would need to provide answers to all these problems.

Object in focus: Obstetrics bag
Visit any doctor or GP surgery across the land and no two will be exactly the same. This is the same with doctor’s bags. While the Gladstone bag might be the quintessential doctor’s bag, the reality was each bag was unique, a snapshot of the mind, personality and challenges of each doctor.
This midwifery bag would be used to supplement their regular bag when a doctor would be called out or have to assist a midwife. Going by the label on a stained apron, this bag seems to have been used by ‘Mary M. Pratt’ but a tin of tools by 'Dr J.G. O’Sullivan’ is also present.
While we don't know much about these names, the bags act in a small way as a biography. They record the challenges and the stressful nights the doctor would no doubt endure, guiding labour or waiting for the flying squad to arrive. In their way, they tell the story of a pragmatic and sensible doctor. An old dried milk tin holds the scissors and tweezers, while an old snuff tin provides the perfect case for suture needles. The objects provide a tantalising glimpse into another life and the doctor’s visits.
Listen to the collection
Dennis Cox recounts how travel possesses its own challenges, from staying in communication to the weather itself.

Object in focus: BT telephone card
Nowadays, finding an address is made simple with smartphones. But this was not always possible.
In the 1970s, only 35% of households had a landline so if a doctor wanted to make contact with the surgery their only hope might be using a nearby phone box with a bag of pennies. The 1980s saw a slightly more high tech solution: the BT Phonecard like this one.
BT Phonecards were introduced in 1980 and allowed doctors to carry a prepaid amount to be used at phone boxes. Households with landlines had increased to 73%, but being able to use them was not always guaranteed, so a phonecard like this provided a trusty backup.
But that is only if the GP wanted to call someone else. If anything needed passing on, they had to hope their secretary (or often a family member roped into the role) knew their route and could call ahead to the location they were visiting to pass on the information.
Although seemingly small, these challenges could have a big impact during the day. The advent of smartphones has seen these challenges disappear along with paper maps, lists of phone numbers and heavy bags of coins that were once so necessary.
Snapshots from the archive
Home visits provided their own challenges for doctors, as the archive shows, such as the sheer distance to travel or even how the doctor travelled. Doctors were often quick to welcome different forms of transport to reach their patients, from trusted horses to new-fangled bicycles.
"I was to provide my own car to be maintained at my own expense, but 9/10ths of petrol was paid by the practice. My accommodation was free, both rent and rates, but I paid a proportion of heat and light bills. Again, no cars had been built during the war, but production of 1939 designs was just starting and cars were available for people with approved needs, such as GP's Petrol, unobtainable by the ordinary person, was also supplied by a special ration book for GPs.
"After successful application for a permit, I obtained an Austin 8 horsepower, costing £125, (only available in black) with my first overdraft. It would be considered today to be totally unsuitable for a country practice, but it stood up to it well, covering an enormous mileage in the process. In those days, cars were serviced every one or two weeks. Dr. A. had a large pre-war American Hudson, which drank petrol and which he drove round the country roads at terrifying speeds, occasionally climbing the banking or half in the ditch when suddenly confronted by another vehicle. Luckily there were very few! A truly fearless driver. Fifty to one hundred and fifty miles a day was quite usual. The practice covered a vast country area which included small hamlets, farmhouses and cottages, and extended to two branch surgeries, which were each manned a real headache because of the mileage involved in having to back-track. Lunch, sandwiches and coffee, in a quiet country lane could be very pleasant.
"Now and again you "borrowed" a patient's phone(and there were not many) to phone back and order the medicines from Mrs. A. These were put on buses to pre-ordained places, usually pubs near their homes, which the patient would call for. 'The Gold Cross'' was a favourite. There was no charge for this and one very quickly picked up the bus times and the locations for each district. Most patients and Mrs. A. knew them anyway. At base, Mrs. seemed to have an inexhaustible supply of friendly people who would take the medication goods to the right bus-stop or terminal where the driver accepted them without a qualm. The system worked very well and it was most unusual for anything to go wrong. The pub or shop owner concerned accepted their part in this also without a qualm and would occasionally take the goods on to a patient's house. Nobody thought this odd. It would probably be illegal today, or does anybody still do it?"
"Now these young fellows had their bicycles. Handy they were he didn't deny, but oh was a loss of dignity. He thought himself with some satisfaction proud of his horse flesh. How he did love his horses - Betty, the best of the lot. His friends wanted to call her Stella from the White Star on her forehead. But Betty it was and no one knew the reason.
"He thought of the shiny top hats, tan breaches and black coat. The thought of bowling along in his smart gig, When it was too hot to ride, the snow with all its glamour of the sleigh."
"The new NHS enabled me, in the backstreets of a slum, to bring to the patient all the benefits of the welfare state. Our hours of consultation, our prescribing, our deputising arrangements were all supervised by the Executive Council, but a very co-operative administrator caused us no aggravation and the terms were reasonable indeed. Overnight the need for bookkeeping disappeared as did the debt collectors. Cost was no longer of importance and I need no longer hesitate in calling out my consultant colleagues. There was no longer the whispered discussion on the doorstep as to how much the patients could afford, if anything, and the almoners disappeared as a means of collecting money in hospital and reappeared in their true role as distributors of help and largesse. Surgery started at 8.30am to 10.30am and this was after I had done my early morning visits out with the milkman. There was no break from visits except for a hurried lunch until I came in at 6pm to take the evening surgery till 8.30pm. I had to have the barber come to the house to cut my hair and in summer a run in the car to Cheadle to buy some fish and chips was a pleasure indeed."
"The country doctor, not so young as all that stood gazing out of the window of a remote farm faced with a dilemma. He had made the pace over the three miles rough road uphill to see an elderly woman was said to be in great abdominal pain and he was heated and not little livid and perplexed.
"She had a breast removed for cancer two years ago and now she had probably secondaries in her spine as the pain was due to a full bladder.
"He was faced with a long walk home to fetch a catheter or a long wait until the husband did the journey and what he minded more two hours increasing pain for his patient then still at the window a thought struck him as he saw a few geese quietly gazing. In the pasture. He sent the husband for some quills, carefully fashioned to his relief and the patients it worked quite well as a catheter."
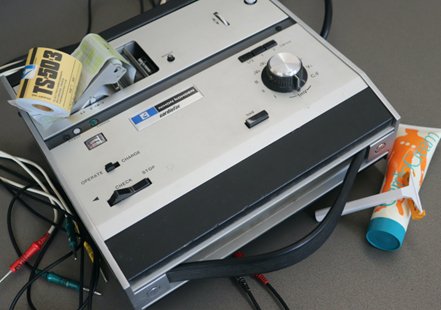
Object in focus: ECG
The electrocardiography machine (ECG) has long been a brilliant test allowing doctors to quickly and accurately understand a patient’s cardiac cycles or heart. Indeed, the first ECGs are probably older than you think, invented almost over 100 years ago in 1895 by Willem Einthoven.
This ECG machine is substantially more recent, produced in the 1980s but represents a new breakthrough of its own. The 1980s saw the development and widespread adoption of portable ECG machines by GPs. These allowed doctors to understand a patient's condition more quickly and if hospital treatment was necessary.
But while such tools were excellent in theory, the reality was often different. They were large and bulky, requiring a bag of their own. As important pieces of equipment, they were often under lock and key. Faced with a patient in an emergency, a doctor would need to make the quick decision of whether taking the extra steps would be worth it. In a city this might make little difference, but in a rural area where ambulance lead times are longer, this small decision could have life-changing consequences.
Thank you for your feedback. Your response will help improve this page.